FELIZ AÑO 2015 PARA TODOS LOS SEGUIDORES Y LECTORES DE ESTE BLOG OS DESEA CON AFECTO, VUESTRO AMIGO, EL PROF. ANTONIO GARFIA.
sábado, 27 de diciembre de 2014
viernes, 26 de septiembre de 2014
CASO 141.- POSTMORTEM DIAGNOSIS OF PALUDISM IN FORENSIC PATHOLOGY. PROF. GARFIA.A
CASO 141
EL DIAGNÓSTICO POSTMORTEM DE PALUDISMO EN PATOLOGÍA FORENSE.
PROF. GARFIA.A
CASE 141
POSTMORTALE DIAGNOSE EINER MALARIA TROPICA.
PROF. GARFIA.A
INTRODUCTION
DESCRIPCIÓN DEL CASO
Antecedentes.-
BAZO
En el estudio del fragmento enviado se evidenció, macroscópicamente, una mala delimitación de las pulpas roja y blanca. La fotografía corresponde a un vaso venoso de la pulpa roja en cuya luz se observan escasos elementos celulares, tanto de la serie roja como de la blanca. Los filamentos teñidos de rojo corresponden a trombos de fibrina. Los hematíes se encuentran severamente deformados y presentan aniso y poiquilocitosis. Existen numerosas células del sistema fagocitario mononuclear que contienen un pigmento negro, granuloso, de forma esférica (pigmento palúdico). En la luz vascular también se encuentran hematíes parasitados por parásitos del paludismo. Por fuera de la pared venosa, los senos venosos y los cordones de Billroth ofrecen un aspecto "sucio" por la abundancia de restos celulares, la escasez de elementos sanguíneos y la presencia de filamentos de fibrina.
Tricrómico de Masson.
FOTO 2.-
En este detalle del contenido vascular venoso -a este aumento- predominan los macrófagos conteniendo pigmento palúdico, en forma de gránulos negros, redondeados, intracitoplasmáticos, así como hematíes que muestran una intensa deformación (aniso y poiquilocitosis), y trombos de fibrina. En el seno de la luz y localizados cerca del endotelio del vaso -aproximadamente a las 5 de la esfera horaria- se encuentran dos merozoítos (formaciones redondeadas a ovaladas, que miden de 0.5 a 1.5 micras de diámetro. Con el colorante de Giemsa el parásito posee citoplasma basófilo, azul pálido, y un punto excéntrico de color rojo oscuro que puede corresponder al núcleo).
BAZO
El aspecto de la pulpa blanca
Algunos de los constituyentes de la pulpa blanca, es decir, los folículos de Maphigio, denominados vainas linfoides periarteriolares por algunos autores, presentaban el aspecto mostrado en esta fotografía.
En ella se puede observar que los linfocitos de la vaina han desaparecido y, en su lugar, se distingue un depósito de material amorfo y morfología nodular, con aspecto necrótico y coloración verdosa, cuyas sombras remedan la morfología de los elementos formes leucocitarios y sus precursores. Se trata de un Microinfarto folicular.
En el seno de la luz de la arteriola central del folículo se detectan trombos de fibrina. La luz del vaso se encuentra fuertemente dilatada y existe adelgazamiento de la pared.
BAZO. ARTERIA TRABECULAR Y RAMAS.-
En el seno de la pulpa roja, esta arteria trabecular y sus ramas transportan escasos elementos formes sanguíneos. En su luz se observan abundantes trombos de fibrina, así como trofozoitos parasitarios. En la pulpa roja se puede distiguir la gran deformación y variabilidad en el tamaño y en la forma de los hematíes. Abundan las formas trofozoíticas.
A este aumento, lo que llama la atención es la presencia de numerosas células que contienen el pigmento palúdico. Se trata de las células de Kupffer que tapizan los capilares sinusoides hepáticos, las cuales pertenecen al Sistema Fagocitario Mononuclear. Algunos hepatocitos muestran depósitos pigmentarios de hierro, teñidos en azul con el método de Perl. No obstante, el pigmento palúdico no produce la reacción del hierro trivalente, aunque la hemozoína -o la hematina- se parezca, químicamente, a la hemosiderina.
La hematina, "in vitro", se produce fácilmente por la acción de los ácido o los álcalis concentrados sobre la hemoglobina. En el organismo, no se produce normalmente en el proceso de transformación de la hemoglobina a otros pigmentos, aunque en casos raros se produce después de crisis hemolíticas intensas, independientemente de su origen. Por lo tanto, el pigmento palúdico parece guardar una estrecha relación con la hematina (hematina+proteína).
Sinonimia:
Pigmento malárico
Pigmento palúdico
Palustre (latín, paluster/tris=pantano o que vive en lugares pantanosos).
Hemozoína.
A mayor aumento se observa la morfología del pigmento palúdico, que constituye agregados esféricos de diferente tamaño, en el citoplasma de las células de Kupffer. Existen depósitos granulares de hierro en los hepatocitos, que se tiñen de color azul con la técnica de Perl.
Los núcleos se tiñeron con Rojo Nuclear.
Existe una necrosis centrolobulillar hepática, observable en esta fotografía, shock- dependiente.
El hígado puede presentar dos formas de necrosis hepatocelular en el curso de un shock: la primera de ellas suele afectar a hepatocitos individualmente y/o a pequeños grupos (necrosis hepatocitaria aislada o necrosis grupal); ésta se distribuye al azar en el seno de los lobulillos sin adoptar nigún patrón morfológico reconocible. La segunda forma es la necrosis centrolobulillar; ésta, suele comenzar con la disociación hepatocitaria y la ruptura del patrón laminar en el centro de los lobulillos hepáticos. Si el estado de shock se prolonga, la necrosis centrolobuillar se extiende hacia la periferia de los lobulillos ( hacia los espacios porta) y adopta un patrón de necrosis centrolobulillar confluente, como podremos ver que sucedió en este caso. Es necesario establecer el diagnóstico diferencial con la autólisis cadavérica, en casos de autólisis avanzada en cadáveres de varios días. El diagnóstico diferencial entre un hígado de shock y una congestión pasiva crónica hepática puede ser difícil. La ausencia de congestión centrolobulillar y la presencia de microtrombos de fibrina en los sinusoides y en las ramas de la vena porta, pueden servir al diagnóstico. A veces, se puede encontrar un hígado de shock en el curso de una congestión pasiva crónica hepática, para terminar de complicar el cuadro.
Es un detalle de la vena centrolobulillar para la demostración de la necrosis de coagulación de los numerosos hepatocitos que circundan la vena. Algunos de ellos contienen abundante pigmentación parda citoplasmática, tal como se observa en la lipofuscinosis centrolobulillar de los consumidores crónicos de algunos fármacos.
En el pulmón, aparte del edema alveolar, lo que llama la atención es la presencia de cuerpos esféricos y/o poligonales, algunos de ellos midiendo más de 200 micras de diámetro, teñidos de color rojizo con el tricrómico de Masson, que circulan por algunos vasos. Son los denominados cuerpos de shock (globular clots), aunque, en algunos casos impresionan como seudomacrocitos (eritrocitos inmaduros).
Cuerpos de Shock o Eritrocitos inmaduros? Detalle.
Algunos de estos cuerpos presentan forma ovalada y ofrecen el aspecto de un huevo parasitario, con opérculo incluido.
En el pulmón se detectó una bronconeumonía, en fase exudativa, mediada por leucocitos polimorfonucleares.
Detalle del exudado multialveolar, así como de un Cuerpo de Creola.
Algunos macrófagos, presentes en el exudado alveolar, conteniendo, también, pigmento palúdico.
Macrófago sanguíneo repleto de pigmento palúdico.
En este frotis, de sangre cadavérica, se puede ver un macrófago/monocito, cargado de pigmento palúdico, y abajo a la izquierda, un esquizonte parasitario repleto de merozoítos. Para el estudio de parásitos en sangre recomiendan los especialisas en paludismo , además del frotis, un estudio de la sangre sobre gota gruesa. Giemsa.
Otro macrófago, repleto de pigmento palúdico, en la sangre circulante. Abajo, a la derecha, bacterias de contaminación.
La imagen superior muestra un esquizonte, repleto de merozoítos, adoptando una disposición en roseta; en el centro, hay pigmento palúdico. En la sangre circulante se pueden detectar tres formas parasitarias: trofozoítos, esquizontes, y gametocitos.
La imagen del centro corresponde a un gametocito presentando un citoplasma voluminoso, de color azul.
La necrosis subendocárdica parcheada shock-dependiente se pone de manifiesto por la presencia de grupos de miocardiocitos que presentan necrosis de coagulación; las miocardiocitos necróticos muestran, además, microvesiculación citoplasmática, probablemente de origen mitocondrial. Cuando las fibras se disponen en secciones longitudinales se detectan numerosas bandas de hipercontracción de naturaleza hipóxica/isquémica.
La coloración tricrómica pone de manifiesto, claramente, la distribución parcheada de las fibras miocárdicas en fase de hipoxia-isquemia, irreversible, las cuales muestran una intensa fucsinofilia.
La presencia de megacariocitos -con núcleos desnudos- circulando en los capilares de los septos alveolares pumonares, es un hallazgo que se presenta en uno de cada tres casos de muerte por shock. La salida de los megacariocitos de la médula ósea es, probablemente, una consecuencia de la hipoxia tisular shock dependiente.
Los denominados cuerpos de shock detectados en el lecho vascular pulmonar, descritos más arriba.
Conclusiones
Los hallazgos histomorfológicos apoyan el diagnóstico de muerte por shock, secundario a accidente de tráfico, en un sujeto afecto de paludismo que fue descubierto durante la necropsia.
EL DIAGNÓSTICO POSTMORTEM DE PALUDISMO EN PATOLOGÍA FORENSE.
PROF. GARFIA.A
CASE 141
POSTMORTALE DIAGNOSE EINER MALARIA TROPICA.
PROF. GARFIA.A
INTRODUCTION
Because of the popularity of long-haul tourism and also to the immigration problems in Europe -and particulary in South Spain- cases of imported paludism are increasingly frequent and, in view of the insidiously progressive course of the disease, it should always be considered in the differential diagnosis. In cases of unexplained death of people from Africans countries, if there is any suspicion of malaria, blood should always be taken for appropiate investigation, in addition to organ samples for histological examination and study. The absolute diagnosis depends on demonstration of the parasite in the stained smear (also the malaria immunofluorescence test on serum). The presence of periodic attack of chills and fever without apparent cause always is suggestive, particulary if the individual has been in a malarious area within the past year and if splenic enlargement is found. The W.B.C. usually is normal or only slightly elevated, with an increased in the percentage of lymphocytes and monocytes.
DESCRIPCIÓN DEL CASO
Antecedentes.-
Conozco escasos datos de la historia de este paciente, varón de 52 años, marinero de profesión, que sufrió un accidente de tráfico en Angola que le provocó numerosas fracturas costales. Fue intervenido de vesícula biliar muriendo en un un Hospital de referencia de Andalucía a consecuencia de un fracaso multiorgánico.
Durante la Autopsia Médico-Legal se puso de manifiesto un derrame pleural izquierdo de casi un litro de líquido de aspecto hemático. Carezco de información de los hallazgos de autopsia, así como de los datos de la historia hospitalaria.
ESTUDIO HISTOPATOLÓGICO
BAZO
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 1. BAZO. PROF. GARFIA.A (hacer click sobre la imagen) |
Tricrómico de Masson.
 | |
|
En este detalle del contenido vascular venoso -a este aumento- predominan los macrófagos conteniendo pigmento palúdico, en forma de gránulos negros, redondeados, intracitoplasmáticos, así como hematíes que muestran una intensa deformación (aniso y poiquilocitosis), y trombos de fibrina. En el seno de la luz y localizados cerca del endotelio del vaso -aproximadamente a las 5 de la esfera horaria- se encuentran dos merozoítos (formaciones redondeadas a ovaladas, que miden de 0.5 a 1.5 micras de diámetro. Con el colorante de Giemsa el parásito posee citoplasma basófilo, azul pálido, y un punto excéntrico de color rojo oscuro que puede corresponder al núcleo).
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 3. DETALLE. BAZO. PROF. GARFIA.A |
BAZO
El aspecto de la pulpa blanca
Algunos de los constituyentes de la pulpa blanca, es decir, los folículos de Maphigio, denominados vainas linfoides periarteriolares por algunos autores, presentaban el aspecto mostrado en esta fotografía.
En ella se puede observar que los linfocitos de la vaina han desaparecido y, en su lugar, se distingue un depósito de material amorfo y morfología nodular, con aspecto necrótico y coloración verdosa, cuyas sombras remedan la morfología de los elementos formes leucocitarios y sus precursores. Se trata de un Microinfarto folicular.
En el seno de la luz de la arteriola central del folículo se detectan trombos de fibrina. La luz del vaso se encuentra fuertemente dilatada y existe adelgazamiento de la pared.
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 4. DETALLE. BAZO. PROF. GARFIA.A |
En el seno de la pulpa roja, esta arteria trabecular y sus ramas transportan escasos elementos formes sanguíneos. En su luz se observan abundantes trombos de fibrina, así como trofozoitos parasitarios. En la pulpa roja se puede distiguir la gran deformación y variabilidad en el tamaño y en la forma de los hematíes. Abundan las formas trofozoíticas.
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 5. HÌGADO. PERL. PROF. GARFIA.A |
A este aumento, lo que llama la atención es la presencia de numerosas células que contienen el pigmento palúdico. Se trata de las células de Kupffer que tapizan los capilares sinusoides hepáticos, las cuales pertenecen al Sistema Fagocitario Mononuclear. Algunos hepatocitos muestran depósitos pigmentarios de hierro, teñidos en azul con el método de Perl. No obstante, el pigmento palúdico no produce la reacción del hierro trivalente, aunque la hemozoína -o la hematina- se parezca, químicamente, a la hemosiderina.
La hematina, "in vitro", se produce fácilmente por la acción de los ácido o los álcalis concentrados sobre la hemoglobina. En el organismo, no se produce normalmente en el proceso de transformación de la hemoglobina a otros pigmentos, aunque en casos raros se produce después de crisis hemolíticas intensas, independientemente de su origen. Por lo tanto, el pigmento palúdico parece guardar una estrecha relación con la hematina (hematina+proteína).
Sinonimia:
Pigmento malárico
Pigmento palúdico
Palustre (latín, paluster/tris=pantano o que vive en lugares pantanosos).
Hemozoína.
 | |
|
Los núcleos se tiñeron con Rojo Nuclear.
 | |
|
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 8. HIGADO. PROF. GARFIA.A |
En la fotografía se observan dos cuerpos esféricos, libres en el seno de un capilar sinusoide hepático, que se tiñen de color azul y presentan pequeñas inclusiones puntiformes citoplasmáticas. La preparación fue teñida con la técnica de Perl para hierro trivalente y parecen corresponder a esquizontes.
 | |
|
El hígado puede presentar dos formas de necrosis hepatocelular en el curso de un shock: la primera de ellas suele afectar a hepatocitos individualmente y/o a pequeños grupos (necrosis hepatocitaria aislada o necrosis grupal); ésta se distribuye al azar en el seno de los lobulillos sin adoptar nigún patrón morfológico reconocible. La segunda forma es la necrosis centrolobulillar; ésta, suele comenzar con la disociación hepatocitaria y la ruptura del patrón laminar en el centro de los lobulillos hepáticos. Si el estado de shock se prolonga, la necrosis centrolobuillar se extiende hacia la periferia de los lobulillos ( hacia los espacios porta) y adopta un patrón de necrosis centrolobulillar confluente, como podremos ver que sucedió en este caso. Es necesario establecer el diagnóstico diferencial con la autólisis cadavérica, en casos de autólisis avanzada en cadáveres de varios días. El diagnóstico diferencial entre un hígado de shock y una congestión pasiva crónica hepática puede ser difícil. La ausencia de congestión centrolobulillar y la presencia de microtrombos de fibrina en los sinusoides y en las ramas de la vena porta, pueden servir al diagnóstico. A veces, se puede encontrar un hígado de shock en el curso de una congestión pasiva crónica hepática, para terminar de complicar el cuadro.
 | |
|
 | |
|
Algunas células de Kupffer también contienen pigmento palúdico. Hem-eos.
 | |
|
Detalle de la necrosis de coagulación centrolobulillar. Técnica de Perl.
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 13 . PULMÓN. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 14 . PULMÓN. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 15 . PULMÓN. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 16 . PULMÓN. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 17 . PULMÓN. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 18 . PULMÓN. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 19 . SANGRE CADAVÉRICA. GIEMSA. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 20. SANGRE CADAVÉRICA. FROTIS. GIEMSA PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 21. SANGRE CADAVÉRICA. FROTIS. GIEMSA. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 22 . SANGRE CADAVÉRICA. FROTIS. GIEMSA. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 23. SANGRE CADAVÉRICA. FROTIS. GIEMSA. PROF. GARFIA.A |
LOS HALLAZGOS MORFOLÓGICOS POSTMORTALES INDICATIVOS DE ESTADO DE SHOCK -Y SUPERVIVENCIA DE HORAS- PREVIO A LA MUERTE.
(MUERTE ESPERADA, RETARDADA O DIFERIDA, NO SÚBITA).
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 24 . CORAZÓN. ENDOCARDIO. HISTOPATOLOGÍA DEL SHOCK. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 25 . CORAZÓN. ENDOCARDIO. HISTOPATOLOGÍA DEL SHOCK. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 26 . HÍGADO DE SHOCK. NECROSIS CENTROLOBULILLAR CONFLUENTE. HISTOPATOLOGÍA DEL SHOCK. PROF. GARFIA.A Es la imagen, a pequeño aumento, de la necrosis centrolobulillar confluente, shock-dependiente. |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 27. PULMÓN. MEGACARIOCITOS EN ALGUNOS CAPILARES ALVEOLARES. HISTOPATOLOGÍA DEL SHOCK. PROF. GARFIA.A |
 |
| CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM. FOTO 28 PULMÓN. GRANDES CUERPOS DE SHOCK. (GLOBULAR CLOTS). HISTOPATOLOGÍA DEL SHOCK.PROF. GARFIA.A |
 |
CASO 141. PALUDISMO. FORENSIC PATHOLOGY FORUM . FOTO 29 . PULMÓN. CUERPO DE SHOCK ( CON ASPECTO DE UN HUEVO PARASITARIO CON OPÉRCULO) HISTOPATOLOGÍA DEL SHOCK. PROF. GARFIA.A |
Conclusiones
Los hallazgos histomorfológicos apoyan el diagnóstico de muerte por shock, secundario a accidente de tráfico, en un sujeto afecto de paludismo que fue descubierto durante la necropsia.
miércoles, 24 de septiembre de 2014
CASE 140. INTESTINAL ISCHEMIA INDUCED BY COCAINE-ALCOHOL ABUSE. PROF. GARFIA.A
CASE 140
VASCULAR LESIONS IN INTESTINAL ISCHEMIA INDUCED BY COCAINE-ALCOHOL ABUSE: REPORT OF A FATAL CASE DUE TO OVERDOSE.
PROF. GARFIA.A
KEY WORDS:
COCAINE, ALCOHOL, SUDDEN DEAH, INTESTINAL ISCHEMIA, VASCULAR LESIONS, INTESTINAL ARTERIOLOPATHY, WEEK-END DEATH.
Bibliografía
Garfia.A.
Lesiones vasculares en la isquemia intestinal asociada al abuso de Cocaína y Alcohol. A propósito de un caso mortal.
IV Jornadas Anuales de Medicina Legal y Forense. Cádiz . 19-21 Abril. 1990.
VASCULAR LESIONS IN INTESTINAL ISCHEMIA INDUCED BY COCAINE-ALCOHOL ABUSE: REPORT OF A FATAL CASE DUE TO OVERDOSE.
PROF. GARFIA.A
KEY WORDS:
COCAINE, ALCOHOL, SUDDEN DEAH, INTESTINAL ISCHEMIA, VASCULAR LESIONS, INTESTINAL ARTERIOLOPATHY, WEEK-END DEATH.
La isquemia intestinal secundaria al abuso de cocaína es una complicación rara. En la literatura se han descrito, hasta la fecha, muy pocos casos.
El diagnóstico de isquemia intestinal se deberá sospechar en personas jóvenes, y/o de mediana edad, adictas a la cocaína que presenten un cuadro de abdomen agudo en un servicio de Urgencias.
La existencia de lesiones vasculares intestinales no se ha confirmado en ninguno de los casos publicados. Macroscópicamente, las lesiones isquémicas son segmentarias y se desconoce si este hecho depende de la dosis ingerida, de la vía de administración, o de la asociación con otras drogas o con el alcohol, como sucedió en este caso.
En este caso describo las lesiones histopatológicas detectadas en las arteriolas submucosas del intestino delgado de un individuo fallecido a consecuencia de una sobredosis de cocaína, asociada a la ingesta de alcohol, el cual presentó durante la autopsia lesiones isquémicas hemorrágicas intestinales segmentarias.
La muerte ocurrió durante un fin de semana y fue presenciada por un testigo.
 | |||||
| Histopatologia Forense Práctica. Caso 140. Foto 1 Prof. Garfia.A (click on the image) |
 |
| Histopatologia Forense Práctica. Caso 140. Foto 2 Prof. Garfia.A (click on the image) Fig. 2.-Nótese, en esta fotografía, la severa contracción - y la estenosis de la luz - de la musculatura lisa que conforma la capa media de la pared arteriolar, si se compara con el aspecto morfológico observado en la arteriola normal en estado relajado. |
Bibliografía
Garfia.A.
Lesiones vasculares en la isquemia intestinal asociada al abuso de Cocaína y Alcohol. A propósito de un caso mortal.
IV Jornadas Anuales de Medicina Legal y Forense. Cádiz . 19-21 Abril. 1990.
jueves, 5 de junio de 2014
139.- CHROMOPATHOLOGY IN FORENSIC PATHOLOGY. HEARTICTERUS.
CASO 139
CHROMOPATHOLOGY
Con la colaboración de los doctores:
CASE 139.-
COLORS OF LIFE (Bilirubin) AND DEATH (Biliverdin) IN FORENSIC PATHOLOGY.
SYNONYMS:
INTRODUCTION
EPICRISIS
Traffic accident on the 20th of January of 2004 followed of serious thoracic traumatism with multiple costal fractures, bilateral bibasal pulmonary contusion and hemothorax. Fracture of L3. Severe respiratory insufficiency that forced an orotracheal intubation and mechanical ventilation. On the 27th of January a febrile syndrome appears with leucocitosis and alveolar infiltrate in left lung. Pneumonia -that causes sepsis with multiorganic failure-. A continuous venous-venous hemofiltration was practised. The infection worsens until there is a severe multiorganic failure with no response to the treatment. Death taking place on the 5th of February, 17 days after the accident.
ANNOTATIONS IN CLINICAL HISTORY
21-1-04
Personal antecedents: No allergies. No high blood pressure, or diabetes or cardiopathies. Hiperlipemia. No neurological problems. Tendency to sleep. Eupneic. Well perfused. Blood pressure 110/60. Oxigen saturation 96%. Hipoventilation in both bases. Good breath sounds in both hemithorax. Soft and depressible abdomen. Sounds presents. TAC: rib and thoracic traumatism wih volet. Bilateral hemothorax and bilateral pulmonary contusion. Abdominal contusion with gastrocolic distension. Left rib fractures 2nd to 5th.
22-01-04
Bad evolution from the beginning, with necessity of amines administration and orotracheal intubation. It was tried to punction the right spill (quite abundant in TAC) obtaining just a small amount of blood. He has presented desaturation and hypotension since yesterday and suppose it is because of an increse of hemothorax. An abdominal scan is asked for (once it is made, it does not contribute significant findings). We cannot discard, at sight of the evolution, septic picture or abdominal visceral breakage. Pleural drainage is placed straight (mean line axillary and 4th intercostal space) and 600 ml of blood was obtained. Pleurovac is left.
23-1-04
Introduce parenteral diet because there is a digestive intolerance; mechanical ventilation pending evaluation for tracheotomy. It is added DOPA because of diminution of the diuresis.
24-01-04
Diminution of the breath sounds in both bases. Low diuresis with positive balance. Blood pressure 140/70. Cardiac frequency 90'. Enteral feeding and continues with dopamine.
25-01-04
Stabilization of the clinical situation. Noncommitment of the oxygenation or ventilation. Hemodinamically stabilized. Increase of uremia in 104 mg% and creatinemia of 1.40 mg%. No fever or hypotension. The dose of dopamine is increased.
27-01-04
Progressive deterioration in spite of better radiology. No fever. Subicteric. Unstable hemodinamically with tendency to hypotension and oliguria. Compensated metabolic acidosis. Renal insufficiency in increase. Quiet abdomen. Leucocitosis with deviation to the left. Septic shock without clarified center.
TAC of thorax: bilateral but accentuated basal consolidation in hemithorax in relation to added extra pneumonic picture.
28-01-04
Negative cultures. 39º. Very unstable hemodinamically. Renal insufficiency. Analitycal setback. Volume overload. By aspiration of orotracheal sounding a pinky foam with watery density is seen.
29-01-04
Diminution of the breath sounds in right base. X-ray of thorax discret infiltrated in average and later lobe straight without appearance of pleural spill. Scan is requested (it confirms left pleural collection.
30-01-04
No fever. Generalized edemas. Icteric. More stable hemodinamically. Symtoms of important fluid overload. Positive accumulated balance 21 litres. Generalized edemas.
1-02-04
Analisis disfunctions continues to be alarming with severe hepatic disfunction.
2-02-02
Hepatic, renal and cardiocirculatory failures, Generalized edemas. Ictericia. Estafilodermia.
3-02-04
Progressive worsening. Multiorganic failure. Tracheostomy. Venous-venous hemofiltration.
5-02-04
Respiratory, renal, hemodinamic and hepatic failure, persistent. Cardiac failure at 19.30 h.
ABOUT THE BILIVERDIN BILIRUBIN METABOLISM AND HEARTICTERUS.
IS IT THIS CASE REPORT AN OPEN WAY TO THE FOLLOW UP RESEARCH IN CLINICAL PATHOLOGY AND TREATMENT POSSIBILITIES DURING THE ACUTE MYOCARDIAL LESIONS IN HUMANS?
We all depend on molecular oxygen and heme catabolism pigments as bilirubin and biliverdin. About 80% of serum bilirubin is derived from hemoglobin of senescent erythrocytes. The factors contributing to destruction of the circulating erythrocytes are not clear. However, about 120 to 130 days after emerging from the marrow, red cells are phagocyticed by macrophages of the reticuloendothelial system cells located on the spleen, liver and bone marrow.
Hemoglobin appears to undergo scissions of the alfa-methene bridge to give a biliverdin-iron protein bridge complex known as verdohemoglobin (choleglobin) because of its green color. Iron is removed, globin liberated, and the free biliverdin is reduced at the gamma-methene bridge to yield bilirubin. Histochemically, the two pigments (bilirubin and biliverdin) are considered bile pigments.
The free iron combines with an iron-binding protein of the plasma (transferrin) and is transported to storage depots or to bone marrow, where it is used in the synthesis of new hemoglobin. The globin-protein is degraded and returned to the body pool of amino acids.
These changes may be summarized as follow:
Hemoglobin (rupture of alfa-methene bridge) > >verdohemoglobin > biliverdin +iron+globin that following:
Biliverdin > Bilirubin > To liver.
Iron > to plasma (transferrin) > to iron stores.
Globin > to amino acid pool.
In contrast to porphyrins, which contain four pyrrole rings linked by four carbon atoms in a closed-ring system, bile pigments lack one of these carbon atoms and can be pictured as an open-ring system or as a tetrapyrrole chain. The system of numbering the pyrrole rings and methene bridges in the bile pigments is derived from that used for porphyrins.
The role of the Heme Oxigenases (HO).
HO are the rate-limiting enzymes in the catabolic degradation of heme. Heme-oxygenase-1 cleaves the porphyrin macrocycle of heme at the expense of molecular oxygen to release a linear tetrapyrrole biliverdin, carbon monoxide, and free iron. Biliverdin is subsequently reduced by cytosolic biliverdin reductase to form the potent antioxidant bilirubin, three important molecules that have attracted great interest because of their possible role in modulating physiological functions. Three HO (HO-1; HO-2 and HO-3) products of three distinct genes, have been identified so far. HO-1 also known as heat shock protein, is a stress-inducible protein shown to be associated with protection against cellular injury. The inducers of the inducible form of HO, or HO-1, include heme, heavy metals, UV radiation, nitric oxid (NO), and reactive oxygen species (ROS) and tisular hypoxia.
The biological functions of HO-1 are thus believed to be associated with a fundamental adaptation and defensive response against oxidative stress and cellular stress. Acumulating evidence suggest a vital role for HO-1 in both cell growth and cell death, specially involvement of the enzyme in the regulation of apoptosis.
Myocardial HO-1 has been induced by stress in various experimental models suggestin a cardioprotective role for this enzyme. Has been reported that oxidative stress produced by pressure overload in the heart or ischemia-reperfusion in the kidney and in the heart induces HO-1 as a cytoprotective mechanism to preserve the tissues from the stress. Some authors (Raju et al.,2004) have shown that cardioselective overexpression of HO-1 exerts a cardioprotective effect after myocardial ischemia-reperfusion in mice, and this effect is probably mediated via an antiapoptotic action of HO-1.
With regard to the molecular mechanism by which HO-1 blocks apoptosis, three major pahways can be proposed:
1.-Decreased intracellular pro-oxidant levels.
2.-Elevated Co production.
3.- Increased bilirubin levels.
INCREASED BILIRUBIN LEVELS
Bilirubin is an important mediator of the antiapoptotic effect of HO-1. It is the final product of the cleavage of the heme ring that is catalyzed by HO and biliverdin-reductasa, and occurs uniquely in mammals. Bilirubin is reputed to be a potentially toxic agent at high concentrations (i.e.,>1.4 mg/dl; aproximatelly 24 micromol/l, in serum), particularly when it accumulates in the serum of neonates and causes jaundice, in which case substantial deposits in the brain with the resultant kernicterus causing major brin damage. However, bilirubin is considered, by numerous authors, to be a major physiologic antioxidant cytoprotectant. The potent physiologic antioxidant actions of bilirubin acting as an antioxidant, is itself reduced to biliverdin and then recycled by biliverdin reductase back to bilirubin. This redox cycle may constitute the principal physiologic function of bilirubin.
Masini et al (2003), have demonstrated that the pretreatment of rats with hemin, an HO-1 inducer, provide protection against ischemia-reperfudion in an "in vivo" model of focal ischemia-reperfusion in the rat heart. The concerted actions of CO, iron, and biliverdin-bilirubin produced by the activation of HO-1 modulate the free radical-induced IR (ischemia-reperfusion) injury, as shown by the decreased both of the infarct area of the increased of the markers of oxidative stress (malonyldialdehyde and tissue calcium).
LA HISTORIA CLINICA
Epicrisis
Se trataba de un varón, de 69 años, que sufrió un espectacular accidente de tráfico por el que fue ingresado en un Hospital de Referencia.
ANOTACIONES EN LA HISTORIA CLINICA
21-1-2004
22-1-04
23-1-04
24-1-04
25-1-04
27-1-04
28-1-04
29-1-04
30-1-04
1-2-04
2-2-04
3-2-04
5-2-04
LA ANALÍTICA
LA AUTOPSIA MÉDICO-LEGAL
FIG.1.-
EN LA FOTO SE APRECIAN TRES REBANADAS CARDIACAS QUE FUERON OBTENIDAS DURANTE LA NECROPSIA.

BLOG 139. FOTO 2.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA.
PROF. GARFIA.A
FOTO 3.-
FOTO 4.- FOTOGRAFÍA TOMADA A LA ALTURA DEL MÚSCULO PAPILAR POSTERIOR VENTRICULAR IZQUIERDO, EN FRESCO Y DESPUÉS DE LA FIJACIÓN EN FORMOL.
DTT= 1,4 DITHIOTREITOL (C4H10O2S2). DIMERCAPTO-2,3 BUTANEDIOL; DTT;
1,4-DITHIO-DL-THREITOL; CLELAND'S REAGENT; DL-THREO-1,4-DIMERCAPTO-2,3-BUTANEDIOL.
AN EXCELLENT REAGENT FOR MANTAINING SH GROUPS IN REDUCED STATE;
QUANTITATIVELY REDUCES DISULFIDES.
MERCK D5545.
FOTO 8.- REACTIVO PARA OXIDACIÓN Y REDUCCIÓN: REDUCCIÓN DE PROTEÍNAS.
DL-DITHIOTHREITOL. DTT.
DTT= 1,4 DITHIOTREITOL (C4H10O2S2). DIMERCAPTO-2,3 BUTANEDIOL; DTT;
1,4-DITHIO-DL-THREITOL; CLELAND'S REAGENT; DL-THREO-1,4-DIMERCAPTO-2,3-BUTANEDIOL.
AN EXCELLENT REAGENT FOR MANTAINING SH GROUPS IN REDUCED STATE;
QUANTITATIVELY REDUCES DISULFIDES.
MERCK D5545.
A= AUTOPSIA.
1.-ASPECTO DEL DEPÓSITO DE BILIRRUBINA OBSERVADO DURANTE LA NECROPSIA.
F= FIJACIÓN EN FORMOL AL 10%.
2.-OXIDACIÓN DE LA BILIRRUBINA A BILIVERDINA POR EL FORMALDEHIDO AL 10%.
3.-ASPECTO DE LA PIGMENTACIÓN DESPUÉS DE LA REDUCCIÓN EN DTT DURANTE 12 HORAS. NÓTESE EL VIRADO DEL COLOR VERDE AL AMARILLENTO POR LA REDUCCIÓN DE LA BILIVERDINA A BILIRRUBINA.
4.- DESPUÉS DE 24 HORAS EN DTT, EL COLOR AMARILLENTO SE HACE MÁS EVIDENTE.
LA INVESTIGACIÓN MICROSCÓPICA
FOTO Nº 12.- A ESTE AUMENTO SE PUEDE COMPROBAR -MEJOR- QUE EL PATRÓN MICROSCÓPICO DEL DEPÓSITO PIGMENTARIO ESTÁ FORMADO POR TEJIDO ESFEROIDAL CONFLUENTE QUE POSEE UN ASPECTO MORFOLÓGICO SIMILAR AL QUE ADOPTAN LOS FOLÍCULOS LINFOIDES DEL TEJIDO LINFOIDE NODULAR.
A LA IZQUIERDA DEL CAMPO, EL EPICARDIO. HACIA LA DERECHA, EL ENDOCARDIO.
PROF. GARFIA.A
LA SORPRESA
FOTO 18.-
LA MIOCARDITIS AGUDA
FOTO 14.-
JUNTO A LA FRONTERA DEL ÁREA NECRÓTICA -EN EL INTERSTICIO MIOCÁRDICO- SE PUEDE VER LA APROXIMACIÓN LEUCOCITARIA, EN FORMA DE COLUMNA QUE CAMINA POR EL TEJIDO CONECTIVO INTERSTICIAL, HACIA LAS 12 DE LA ESFERA HORARIA.
MIOCARDITIS AGUDA
FOTO 13.-
LA COLUMNA LEUCOCITARIA INFILTRANDO EL TEJIDO CONECTIVO PERINECRÓTICO.
EN LOS MÁRGENES DE LA NECROSIS MIOCÁRDICA LOS MIOCARDIOCITOS SUPERVIVVIENTES, SEPARADOS ENTRE SÍ POR EDEMA INTERSTICIAL.
EN AZUL, LAS BANDAS O LÍNEAS DE UNIÓN DESMOSÓMICAS (LÍNEAS Z).
MIOCARDITIS AGUDA
EN LA FRONTERA DE LA NECROSIS
FOTO 23.-
EN EL FOCO DE NECROSIS.
M
FOTO 25 .-
SE VEN ALGUNAS BANDAS DE CONTRACCIÓN Y RESTOS DE LA ESTRIACIÓN EN ALGUNOS MIOCARDIOCITOS. PREDOMINA LA INTENSA BASOFILIA EN LA MAYORÍA DE LOS MIOCARDIOCITOS NECRÓTICOS.
FOTO 26.-
EN EL CENTRO DEL ÁREA NECRÓTICA SE CONSERVA UN MIOCARDIOCITO QUE PRESENTA BANDAS DE HIPERCONTRACCIÓN EOSINÓFILAS EN EL CITOPLASMA.
FOTO 27.- LA COMPOSICIÓN QUIERE MOSTRAR EL ASPECTO MICROSCÓPICO QUE SE OBSERVA EN LAS ÁREAS MACROSCÓPICAS MUESTREADAS QUE SE INDICAN EN LA FOTOGRAFÍA.
FOTO 29.-
DEPÓSITOS DE BILIRRUBINA SEÑALADOS POR LAS FLECHAS.
M=MIOCARDIOCITOS NECRÓTICOS.
FOTO 30.-
LAS TINCIONES CON HEMATOXILINA-EOSINA-FLOXINA DEMUESTRAN LA NECROSIS DE COAGULACIÓN DE LOS MIOCARDIOCITOS, LA MIOCITOLISIS Y LA PRESENCIA DE INCLUSIONES CITOPLASMÁTICAS BASÓFILAS -ALGUNAS DE LAS CUALES SUGIEREN UNA ETIOLOGÍA BACTERIANA.
BIBLIOGRAFÍA CONSULTADA
Schmorl, G.-
Zur kenntniss der Ikterus Neonatorum, insbesondere der dabei umftretenden Gehirnveranderungen. Verhandlung Deutsche Patologische Gesellschaft. 6: 109. 1903
Fang, J., Akaike, T and Maeda.H
Antiapoptotic role of heme oxygenase (HO) and the potential of HO as a target in anticancer treatment. Apoptosis 2004; 9:27-35.
Turkel SB.-
Autopsy findings associated with neonatal hyperbilirubinemia.
Clin Perinatol. 1990 Ju; 17 (2): 381-396.
Masini, E et al.-
Hme Oxygenase-1 and the Ischemia-Reperfusion Injury in the Rat Heart.
Exp Biol Med 228:546-549, 2003.
Wu TW et al.-
Albumin-bound bilirubins protect human ventricular myocites against oxyradical damage.
Biochem Cell Biol 69: 683-688. 1991.
Raju VS et al.-
Cardioselective overexpression of HO-1 prevents I/R-induced cardiac dysfunction and apoptosis.
Am J Physiol Heart Circ Physiol 283: H688-H694. 2002.
Agradecimientos
A la Dra. María José Haro, por la ayuda prestada en la traducción al inglés.
CHROMOPATHOLOGY
HERZIKTERUS
(ICTERICIA CARDIACA):
(ICTERICIA CARDIACA):
COLORES DE VIDA (Bilirrubínico) Y MUERTE (Biliverdínico) EN PATOLOGÍA FORENSE: A PROPÓSITO DE UN CASO DE ICTERICIA CARDIACA RUBÍNICO- VERDÍNICA.
PROF. GARFIA.
Con la colaboración de los doctores:
SERRATOSA SÁNCHEZ DE IBARGÜEN, Alejandro y
RODRÍGUEZ HORNILLO, Manuel
CASE 139.-
COLORS OF LIFE (Bilirubin) AND DEATH (Biliverdin) IN FORENSIC PATHOLOGY.
HERZIKTERUS
BILIRUBIN-BILIVERDIN REDOX SYSTEM AS AN EVIDENT PHYSIOLOGICAL ANTIOXIDANT CYTOPROTECTIVE SYSTEM IN HUMANS,
AND THEIR POSTMORTEM MORPHOLOGICAL EXPRESSION IN A MYOCARDITIS FATAL CASE -DUE TO SEPSIS- FROM A FORENSIC CASE.
HEARTICTERUS.
HERZIKTERUS.
HERZIKTERUS.
ICTERICIA CARDIACA.
CARDIAC RUBIN-VERDINICTERUS.
HERZ RUBIN-VERDINIKTERUS.
CARDIAC RUBIN-VERDIN COLORS IN A HUMAN CADAVER.
INTRODUCTION
Bilirubin, an abundant pigment causing jaundice, has long lacked any clear physiological role.
Bilirubin arises from enzymatic reduction by biliverdin reductase of biliverdin, a product of heme oxygenase activity. Bilirubin is a potent antioxidant that can protect cells from a 10.000-fold excess of H2O2 "in vitro experiments". Thus, cellular depletion of bilirubin by RNA interference markedly augments tissue levels of reactive oxygen species and causes apoptotic cell death. Depletion of glutathione, generally regarded as a physiologic antioxidant cytoprotectant, elicits lesser increases in reactive oxygen species and cell death. The potent physiologic antioxidant actions of bilirubin reflect an amplification cycle whereby bilirubin, acting as an antioxidant, is itself oxidized to biliverdin and then recycled by biliverdin reductase back to bilirubin. This redox cycle may constitute the principal function of bilirubin.
We report a forensic case where a man died, due to a traffic accident, 17 days post-accident.
The medico-legal autopsy shows a brown-yellowish pigment deposition inside the left ventricular wall of the heart which showed a morphological pattern typical of a myocarditis. The microscopical examination of the pigmentation areas demonstrated an acute circumferential myocardial necrosis of the left ventricular wall (acute myocarditis).
We discuss if the role of the bilirubin in this septic myocarditis case was provide antioxidative cytoprotection to the myocardial necrosis cell adopting a morphological pattern of an acute myocarditis in the course of a sepsis.
The term "Kernikterus" was coined in 1903 by Schmorl, G (etymologicaly from Kern=nucleus, in German, and Ikterus (in anciant latin for jaundice), to describe the selective yellow pigmentation of basal ganglia and brainstem nuclei by bilirubin deposition causing subsequent degeneration (bilirubin encephalopathy). Since then, kernikterus as a clinicopathologic entity, has been described extensively in a number of articles and monographs, but today it is a rather historical disease.
The concept hearticterus (cardiac jaundice), has been created by uns from the desire to describe the "selective" orange-green pigmentation (bilirubin-biliverdin) of myocardial cell necrotic areas, in a case of septic myocarditis secondary to a traffic road accident which was followed by extensive hemorrhage in pleura and peritoneum, multiorganic failure (hepatic, with high levels of blood bilirubin, and renal) and fatal sepsis.
The finding of this selective bilirubin-biliverdin pigmentation deposition "exclusively" in areas where microscopically I found an acute myocardial cell necrosis, which adopts a circumferential pattern inside the mesocardia of the left ventricular wall (septic myocarditis) is appointing that we have discovered that the bilirubin acts as a major physiologic antioxidant cytoprotectant in humans.
Bilirubin, which is highly lipophilic, is associated intimately with cell membranes where it might prevent lipid peroxidation and protect membranes protein of the myocardiocytes damage.
These findings arise the important question of whether hipoxic-ischemic injury plays a role in the development of the lesions of kernicterus and the deposition of bilirubin may be secondary to the neuronal damage and not the primary cause of the bilirubin encephalopathy.
Traffic accident on the 20th of January of 2004 followed of serious thoracic traumatism with multiple costal fractures, bilateral bibasal pulmonary contusion and hemothorax. Fracture of L3. Severe respiratory insufficiency that forced an orotracheal intubation and mechanical ventilation. On the 27th of January a febrile syndrome appears with leucocitosis and alveolar infiltrate in left lung. Pneumonia -that causes sepsis with multiorganic failure-. A continuous venous-venous hemofiltration was practised. The infection worsens until there is a severe multiorganic failure with no response to the treatment. Death taking place on the 5th of February, 17 days after the accident.
ANNOTATIONS IN CLINICAL HISTORY
21-1-04
Personal antecedents: No allergies. No high blood pressure, or diabetes or cardiopathies. Hiperlipemia. No neurological problems. Tendency to sleep. Eupneic. Well perfused. Blood pressure 110/60. Oxigen saturation 96%. Hipoventilation in both bases. Good breath sounds in both hemithorax. Soft and depressible abdomen. Sounds presents. TAC: rib and thoracic traumatism wih volet. Bilateral hemothorax and bilateral pulmonary contusion. Abdominal contusion with gastrocolic distension. Left rib fractures 2nd to 5th.
22-01-04
Bad evolution from the beginning, with necessity of amines administration and orotracheal intubation. It was tried to punction the right spill (quite abundant in TAC) obtaining just a small amount of blood. He has presented desaturation and hypotension since yesterday and suppose it is because of an increse of hemothorax. An abdominal scan is asked for (once it is made, it does not contribute significant findings). We cannot discard, at sight of the evolution, septic picture or abdominal visceral breakage. Pleural drainage is placed straight (mean line axillary and 4th intercostal space) and 600 ml of blood was obtained. Pleurovac is left.
23-1-04
Introduce parenteral diet because there is a digestive intolerance; mechanical ventilation pending evaluation for tracheotomy. It is added DOPA because of diminution of the diuresis.
24-01-04
Diminution of the breath sounds in both bases. Low diuresis with positive balance. Blood pressure 140/70. Cardiac frequency 90'. Enteral feeding and continues with dopamine.
25-01-04
Stabilization of the clinical situation. Noncommitment of the oxygenation or ventilation. Hemodinamically stabilized. Increase of uremia in 104 mg% and creatinemia of 1.40 mg%. No fever or hypotension. The dose of dopamine is increased.
27-01-04
Progressive deterioration in spite of better radiology. No fever. Subicteric. Unstable hemodinamically with tendency to hypotension and oliguria. Compensated metabolic acidosis. Renal insufficiency in increase. Quiet abdomen. Leucocitosis with deviation to the left. Septic shock without clarified center.
TAC of thorax: bilateral but accentuated basal consolidation in hemithorax in relation to added extra pneumonic picture.
28-01-04
Negative cultures. 39º. Very unstable hemodinamically. Renal insufficiency. Analitycal setback. Volume overload. By aspiration of orotracheal sounding a pinky foam with watery density is seen.
29-01-04
Diminution of the breath sounds in right base. X-ray of thorax discret infiltrated in average and later lobe straight without appearance of pleural spill. Scan is requested (it confirms left pleural collection.
30-01-04
No fever. Generalized edemas. Icteric. More stable hemodinamically. Symtoms of important fluid overload. Positive accumulated balance 21 litres. Generalized edemas.
1-02-04
Analisis disfunctions continues to be alarming with severe hepatic disfunction.
2-02-02
Hepatic, renal and cardiocirculatory failures, Generalized edemas. Ictericia. Estafilodermia.
3-02-04
Progressive worsening. Multiorganic failure. Tracheostomy. Venous-venous hemofiltration.
5-02-04
Respiratory, renal, hemodinamic and hepatic failure, persistent. Cardiac failure at 19.30 h.
ABOUT THE BILIVERDIN BILIRUBIN METABOLISM AND HEARTICTERUS.
IS IT THIS CASE REPORT AN OPEN WAY TO THE FOLLOW UP RESEARCH IN CLINICAL PATHOLOGY AND TREATMENT POSSIBILITIES DURING THE ACUTE MYOCARDIAL LESIONS IN HUMANS?
We all depend on molecular oxygen and heme catabolism pigments as bilirubin and biliverdin. About 80% of serum bilirubin is derived from hemoglobin of senescent erythrocytes. The factors contributing to destruction of the circulating erythrocytes are not clear. However, about 120 to 130 days after emerging from the marrow, red cells are phagocyticed by macrophages of the reticuloendothelial system cells located on the spleen, liver and bone marrow.
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. OPTICAL MICROSCOPY. ERYTHROCYTES. GIEMSA STAIN. PROF. GARFIA.A. |
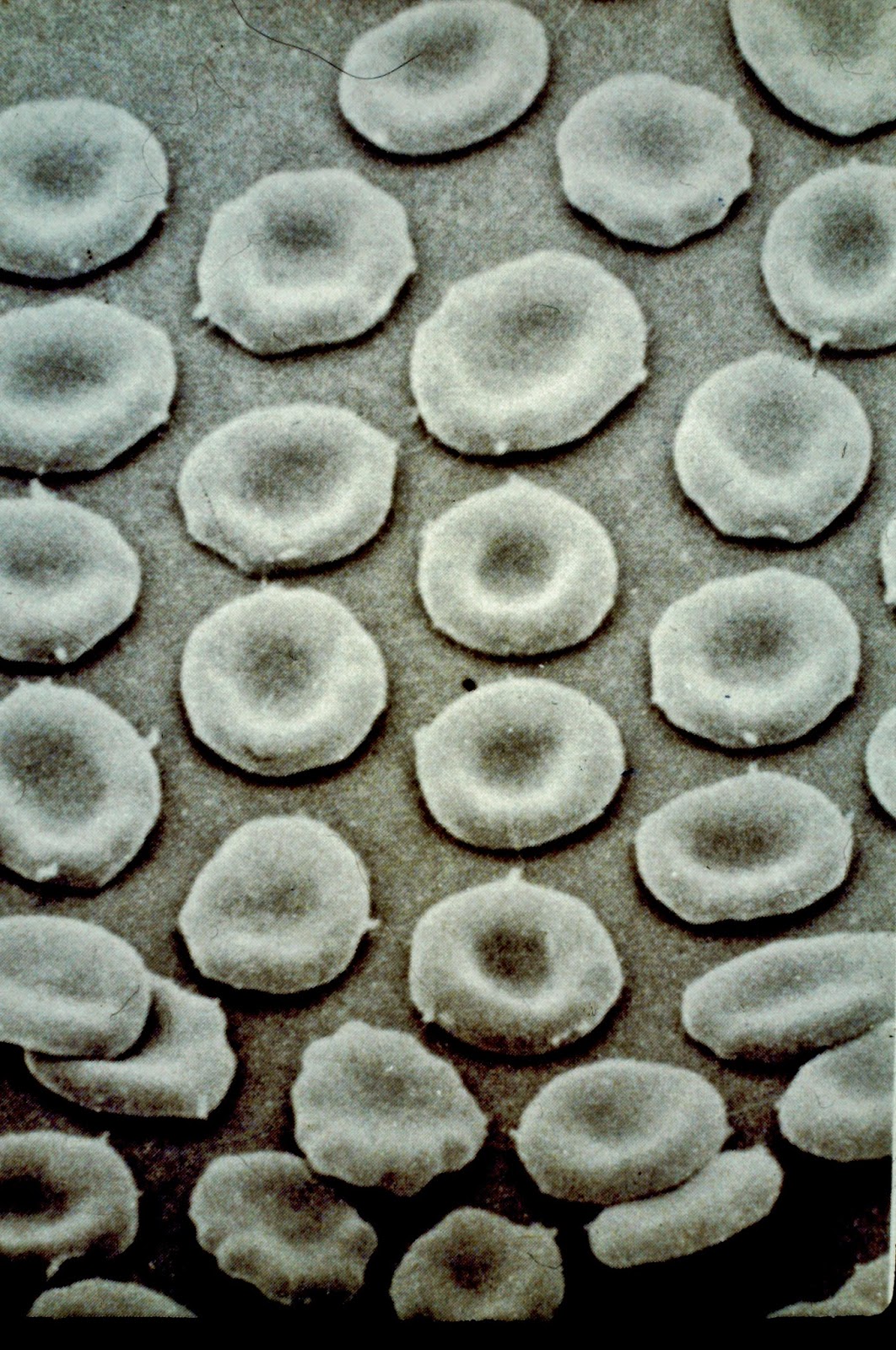 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. ERYTHROCYTES VIEWED WITH SCANNING ELECTRON MICROSCOPE (SEM). PROF. GARFIA.A. |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. HEPATIC SINUSOID WITH ERYTHROCYTES(D). TRANSMISSION ELECTRON MICROSCOPE (TEM). PROF. GARFIA.A. |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A. Ruptura del anillo cerrado tetrapirrólico del grupo Hem de la hemoglobina en el puente alfa-meteno para formar el esqueleto de los pigmentos biliares (bilirrubina y biliverdina). |
Hemoglobin appears to undergo scissions of the alfa-methene bridge to give a biliverdin-iron protein bridge complex known as verdohemoglobin (choleglobin) because of its green color. Iron is removed, globin liberated, and the free biliverdin is reduced at the gamma-methene bridge to yield bilirubin. Histochemically, the two pigments (bilirubin and biliverdin) are considered bile pigments.
The free iron combines with an iron-binding protein of the plasma (transferrin) and is transported to storage depots or to bone marrow, where it is used in the synthesis of new hemoglobin. The globin-protein is degraded and returned to the body pool of amino acids.
These changes may be summarized as follow:
Hemoglobin (rupture of alfa-methene bridge) > >verdohemoglobin > biliverdin +iron+globin that following:
Biliverdin > Bilirubin > To liver.
Iron > to plasma (transferrin) > to iron stores.
Globin > to amino acid pool.
In contrast to porphyrins, which contain four pyrrole rings linked by four carbon atoms in a closed-ring system, bile pigments lack one of these carbon atoms and can be pictured as an open-ring system or as a tetrapyrrole chain. The system of numbering the pyrrole rings and methene bridges in the bile pigments is derived from that used for porphyrins.
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A. |
Bilirubin is transported from the reticuloendothelial system to the liver as a protein complex, either as bilirubin-globulin or as bulirubin-albumin. In the liver the protein is separated, and the bilirubin converted into the corresponding diclunoride (soluble) by reaction with uridindiphosphoglucuronato. The soluble diglucuronide passes into the bili canaliculi and thence into the bile.
HO are the rate-limiting enzymes in the catabolic degradation of heme. Heme-oxygenase-1 cleaves the porphyrin macrocycle of heme at the expense of molecular oxygen to release a linear tetrapyrrole biliverdin, carbon monoxide, and free iron. Biliverdin is subsequently reduced by cytosolic biliverdin reductase to form the potent antioxidant bilirubin, three important molecules that have attracted great interest because of their possible role in modulating physiological functions. Three HO (HO-1; HO-2 and HO-3) products of three distinct genes, have been identified so far. HO-1 also known as heat shock protein, is a stress-inducible protein shown to be associated with protection against cellular injury. The inducers of the inducible form of HO, or HO-1, include heme, heavy metals, UV radiation, nitric oxid (NO), and reactive oxygen species (ROS) and tisular hypoxia.
The biological functions of HO-1 are thus believed to be associated with a fundamental adaptation and defensive response against oxidative stress and cellular stress. Acumulating evidence suggest a vital role for HO-1 in both cell growth and cell death, specially involvement of the enzyme in the regulation of apoptosis.
Myocardial HO-1 has been induced by stress in various experimental models suggestin a cardioprotective role for this enzyme. Has been reported that oxidative stress produced by pressure overload in the heart or ischemia-reperfusion in the kidney and in the heart induces HO-1 as a cytoprotective mechanism to preserve the tissues from the stress. Some authors (Raju et al.,2004) have shown that cardioselective overexpression of HO-1 exerts a cardioprotective effect after myocardial ischemia-reperfusion in mice, and this effect is probably mediated via an antiapoptotic action of HO-1.
With regard to the molecular mechanism by which HO-1 blocks apoptosis, three major pahways can be proposed:
1.-Decreased intracellular pro-oxidant levels.
2.-Elevated Co production.
3.- Increased bilirubin levels.
INCREASED BILIRUBIN LEVELS
Bilirubin is an important mediator of the antiapoptotic effect of HO-1. It is the final product of the cleavage of the heme ring that is catalyzed by HO and biliverdin-reductasa, and occurs uniquely in mammals. Bilirubin is reputed to be a potentially toxic agent at high concentrations (i.e.,>1.4 mg/dl; aproximatelly 24 micromol/l, in serum), particularly when it accumulates in the serum of neonates and causes jaundice, in which case substantial deposits in the brain with the resultant kernicterus causing major brin damage. However, bilirubin is considered, by numerous authors, to be a major physiologic antioxidant cytoprotectant. The potent physiologic antioxidant actions of bilirubin acting as an antioxidant, is itself reduced to biliverdin and then recycled by biliverdin reductase back to bilirubin. This redox cycle may constitute the principal physiologic function of bilirubin.
Masini et al (2003), have demonstrated that the pretreatment of rats with hemin, an HO-1 inducer, provide protection against ischemia-reperfudion in an "in vivo" model of focal ischemia-reperfusion in the rat heart. The concerted actions of CO, iron, and biliverdin-bilirubin produced by the activation of HO-1 modulate the free radical-induced IR (ischemia-reperfusion) injury, as shown by the decreased both of the infarct area of the increased of the markers of oxidative stress (malonyldialdehyde and tissue calcium).
LA HISTORIA CLINICA
Epicrisis
Se trataba de un varón, de 69 años, que sufrió un espectacular accidente de tráfico por el que fue ingresado en un Hospital de Referencia.
Presentaba un traumatismo torácico grave, con múltiples fracturas
costales, contusión pulmonar bibasal y hemotórax bilateral. Existía una
fractura vertebral en L3.
El enfermo se encontraba en insuficiencia respiratoria severa lo
que obligó a llevar a cabo una intubación orotraqueal y ventilación
mecánica.
A
los 7 días del ingreso apareció un síndrome febril -con leucocitosis- e
infiltrado alveolar en el pulmón izquierdo. A la neumonía se le atribuyó
una sepsis seguida de disfunción multiorgánica. Se
llevó a cabo una hemofiltración venosa-venosa, contínua. El cuadro
séptico se agravó hasta la aparición de un fracaso multiorgánico severo,
sin respuesta al tratamiento.
El fallecimiento se produjo a los 17 días del ingreso y se consideró secundario a una parada cardiaca secundaria a un shock séptico y a un fallo multiorgánico.
ANOTACIONES EN LA HISTORIA CLINICA
21-1-2004
Antecedentes personales:
No alergias. Niega HTA, DM y cardiopatías. Hiperlipemia.
Exploración: No déficit neurológico. Tendencia al sueño. Eupneico. Bien perfundido. TA 110/60. Saturación O2: 96%. Hipoventilación de ambas bases pulmonares. Abdomen blando y depresible. Ruidos presentes.
No alergias. Niega HTA, DM y cardiopatías. Hiperlipemia.
Exploración: No déficit neurológico. Tendencia al sueño. Eupneico. Bien perfundido. TA 110/60. Saturación O2: 96%. Hipoventilación de ambas bases pulmonares. Abdomen blando y depresible. Ruidos presentes.
TAC:Traumatismo
torácico con volet costal. Hemotórax bilateral y contusión pulmonar
bilateral. Contusión abdominal con distensión gastrocólica. Fracturas
costales 2ª a 5ª, izquierdas.
22-1-04
Mala evolución desde el ingreso, con necesidad de administración de
aminas y de intubación orotraqueal
Desde
el día anterior ha presentado desaturación e hipotensión y se sospecha
aumento del hemotórax. Se solicita ecografía abdominal (llevada a cabo
no aporta información significativa).
A la vista de la evolución del paciente, no se puede descartar cuadro
séptico o rotura de víscera abdominal. Se coloca drenaje pleural
derecho -línea media axilar y 4º espacio intercostal- y se extraen 600
ml de sangre. Se deja pleurovac.
23-1-04
Dieta parenteral por intolerancia digestiva. Ventilación mecánica.
Pendiente de valoración la realización de traqueostomía. Se añade Dopa,
por disminución de la diuresis.
24-1-04
Disminución del murmullo vesicular en ambas bases. Baja diuresis con
balance positivo. TA 140/70. FC 90x'. Inicia dieta enteral y se continua
la administración de Dopa.
25-1-04
Situación clínica estable. Sin compromiso oxigenación-ventilación. Hemodinámicamente estable. Aumento de la Uremia a 104 mg% (ver gráfico) y de la creatininemia a 1.40 mg%. Sin fiebre ni hipotensión. Se incrementa la dosis de Dopamina.
Deterioro
progresivo a pesar de mejor radiología. Afebril. Subictérico.
Hemodinámicamente inestable con tendencia a hipotensión y oliguria.
Acidosis metabólica compensada. Insuficiencia renal en aumento. Abdomen
quieto.
Leucocitosis con desviación a la izquierda. Shock séptico sin foco aclarado.
(ver gráfico).
TAC
Tórax con consolidación basal bilateral, más acentuada en hemitórax izquierdo, en relación con cuadro neumónico sobreañadido.
TAC
Tórax con consolidación basal bilateral, más acentuada en hemitórax izquierdo, en relación con cuadro neumónico sobreañadido.
28-1-04
Cultivos negativos.
Fiebre (39º). Hemodinámicamente muy inestable. Insuficiencia renal. Descalabro analítico.
A las 14.30, sobrecarga de volumen. Mediante aspiración de sonda
orotraqueal se aprecia salida de espuma sonrosada y densidad acuosa.
Disminución del murmullo vesicular en la base derecha. RX de tórax:
discreto infiltrado en los lóbulos medio y posterior derecho sin
apariencia de derrame pleural.
30-1-04
Afebril.
Edematoso. Ictérico. Hemodinámicamente más estable. Síntomas de
importante sobrecarga de volumen. Balance acumulado positivo de 21
litros. Edemas generalizados a tensión.
1-2-04
Sigue presentando química alarmante con severa disfunción hepática.
2-2-04
Fallos hepático, renal y cardiocirculatorio. Edemas generalizados. Ictericia. Estafilodermia.
3-2-04
Empeoramiento progresivo. Fracaso multiorgánico. Necesidad de traqueostomía. Hemofiltración venosa-venosa contínua.
Fracaso persistente hepático, renal, respiratorio y hemodinámico.
Al atardecer, parada cardiaca seguida de exitus.
Al atardecer, parada cardiaca seguida de exitus.
LA ANALÍTICA
 |
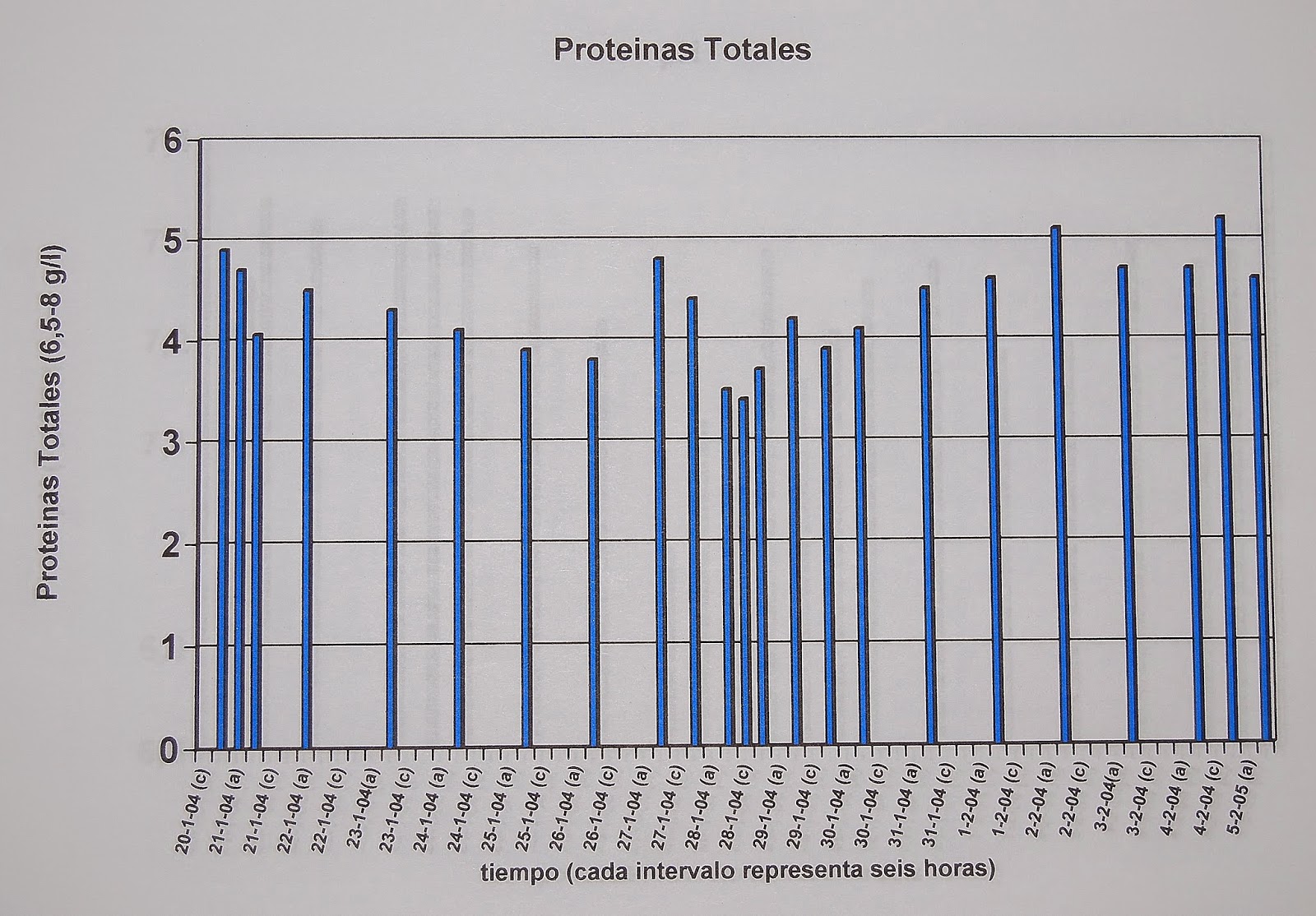
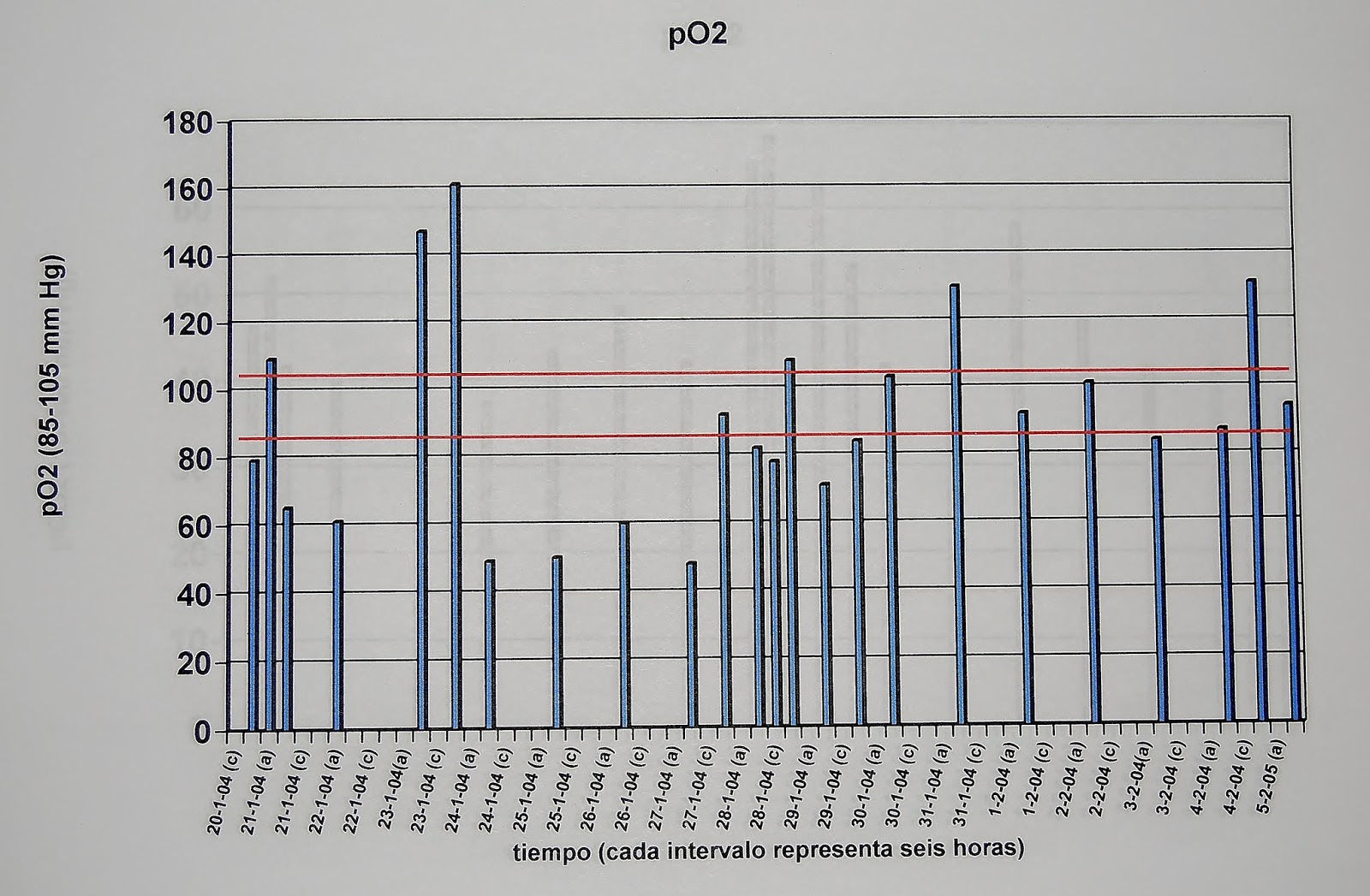
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A. GRAFICO 1 EVOLUCIÓN DE LA BILIRRUBINA TOTAL. Las líneas rojas delimitando el rango de valores normales. |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A. GRAFICO 2 EVOLUCIÓN DE LA BILIRRUBINA TOTAL |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 3 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 4 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 5 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 6 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 7 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 8 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 9 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 10 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 11 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 12 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 13 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 14 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 15 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 16 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 17 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 18 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 19 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 20 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 21 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 22 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 23 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 24 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 25 |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A GRÁFICO 26 |
LA AUTOPSIA MÉDICO-LEGAL
1.-EXAMEN EXTERNO
Se trataba del cadáver de un varón de raza blanca, de edad aparente concordante con la cronológica. Presentaba discreto sobrepeso. Medía 1.80 cm de altura. No se detectaron anomalías somáticas. El cadáver se encontraba desnudo y cubierto con sábana.
La inspección detallada mostró los siguientes hallazgos:
1.-Punturas yatrogénicas inguinales bilaterales, cubiertas con sendos apósitos.
2.-Sonda anal.
3.-Edema intenso escrotal y de las extremidades.
4.-Hematoma submandibular derecho.
5.-Traqueostoma.
6.-Herida suturada en región subaxilar izquierda.
7.-Hematomas en distintas fases evolutivas localizados en regiones mamaria y axilar.
8.- Extenso hematoma en la región iliaca derecha.
9.- Erosiones en manos y regiones maleolares.
10.-Herida inciso-contusa en la región frontal, de unos 10 cm de longitud.
11.- Intenso tinte ictérico en todo el cuerpo.
2.-EXAMEN INTERNO
2.1 Cavidad craneal
Hematoma subgaleal en región frontal.
Encéfalo, congestivo y edematoso, que pesa 1340 g.
Ausencia de fracturas craneales.
2.2 Cavidad torácica
Múltiples fracturas de la parrilla costal que afectan, en el hemitórax derecho, a la 2ª, 3ª,4ª, 5, 6ª, 7ª, 8, 9ª y 10ª.
En el izquierdo se encuentran fracturadas la 2ª, 3ª y 4ª.
Fractura del tercio medio esternal.
Abundantes hematomas intercostales.
Hidrotórax bilateral.
Pulmón izquierdo: 1960 g.
Pulmón derecho: 2100 g.
Ambos presentan, en su cara anterior, varios focos de contusión.
Absceso, de contenido purulento, en el lóbulo inferior del pulmón izquierdo, que mide 2.5x2.9 cm, de diámetros mayores.
Ambos pulmones, al corte, se encuentran hepatizados y edematosos. A la expresión, suave, rezuman abundante líquido, de aspecto sero-hemático y color grisáceo.
Corazón
De 470 g. Presenta discreta hipertrofia ventricular izquierda y, a los cortes en rebanada, muestra un infiltrado, de color pardo amarillento, que se extiende por el espesor mesocárdico del ventrículo izquierdo adoptando un patrón circunferencial (ver foto 1). El ventrículo derecho no muestra este tipo de cambio. Los perímetros valvulares se encuentran dentro del rango normal y las arterias coronarias son permeables y con escasas placas de ateroma.
2.3.-Cavidad abdominal:
Hígado.- Pesa 1900 g. Es friable al tacto y presenta una coloración amarillo-verdosa intensa.
Bazo.-De 200 g, de peso. Es muy friable y presenta, al corte, aspecto en "salsa de tomate".
Riñones.-De 215g (derecho) y 2010 (izquierdo). Presentan, en superficie y al corte, marcada palidez anémica y aspecto de riñones de shock.
Resto de la cavidad abdominal sin hallazgos de interés.
3.-Diagnósticos macroscópicos emitidos en el Informe de Autopsia:
1.-Traumatismo cráneo-encefálico. Herida frontal. Hematoma subgaleal frontal.
2.-Traumatismo torácico grave con diversas fracturas costales y del esternón.
3.-Neumonía bilateral. Absceso pulmonar izquierdo.
4.-Contusiones pleuro-pulmonares.
5.-Hidrotórax bilateral.
6.-Discreta cardiomegalia. Infiltración ventricular izquierda, de coloración pardo amarillenta, circunferencial.
7.-Atrofia hepática aguda.
8.-Riñones de shock.
9.-Bazo séptico.
Conclusiones del Examen Macroscópico:
1.-Causa de la Muerte:
Shock séptico y fracaso multiorgánico
post-accidente de tráfico.
post-accidente de tráfico.
2.-Manera de la Muerte:
Accidental viaria (choque de vehículos).
 |
| BLOG 139. FOTO 1.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FIG.1.-
EN LA FOTO SE APRECIAN TRES REBANADAS CARDIACAS QUE FUERON OBTENIDAS DURANTE LA NECROPSIA.
NÓTESE EL INFILTRADO, DE COLOR AMARILLENTO, QUE SE ENCUENTRA LOCALIZADO EN EL MESOCARDIO, FORMANDO UN ANILLO CIRCUNFERENCIAL, CASI COMPLETO, EN EL ESPESOR DEL VENTRÍCULO IZQUIERDO.
EL INFILTRADO ADOPTA EL PATRÓN MACROSCÓPICO CARACTERÍSTICO DE LAS CICATRICES MIOCÁRDICAS QUE SE OBSERVAN EN LAS MIOCARDITIS CRÓNICAS O CURADAS.
BLOG 139. FOTO 2.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA.
PROF. GARFIA.A
Una de las rebanadas cardiacas después de la fijación en formol comercial ( formol al 10%).
Nótese el virado del color amarillo al verde (bilirrubina-biliverdina), del infiltrado miocárdico ventricular izquierdo. El patrón morfológico de la distribución del infiltrado corresponde al que se observa, en forma de cicatrices miocárdicas blanquecinas, en las miocarditis curadas.
Existe una ausencia total de afectación ventricular derecha.
 |
BLOG 139. FOTO 3.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A
Nótese la afectación del músculo papilar posterior ventricular izquierdo.
|
 |
| BLOG 139. Foto 4.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
LA FOTOGRAFÍA FUE TOMADA DE LA MISMA RODAJA CARDIACA, EN FRESCO, Y MOSTRANDO - A LA IZQUIERDA- LA INFILTRACIÓN AMARILLENTA Y -DESPUÉS DE LA FIJACIÓN EN FORMOL AL 10%- A LA DERECHA; EN ÉSTA SE OBSERVA EL VIRADO AL VERDE DEL INFILTRADO, DESPUÉS DE LA FIJACIÓN EN FORMOL.
 |
| BLOG 139 Foto 5.-. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
 |
| BLOG 139. Foto 6.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FOTO 5.- FOTOGRAFÍAS CORRESPONDIENTES A LA MISMA RODAJA CARDICA CERCANAS AL NIVEL VALVULAR.
AL IGUAL QUE LAS DOS ANTERIORES, FUERON TOMADAS EN FRESCO Y DESPUÉS DE LA FIJACIÓN EN FORMOL.
 |
| BLOG 139. Foto 7.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FOTO 6.- ASPECTO MOSTRADO POR LAS RODAJAS CARDIACAS -DESDE EL NIVEL VALVULAR HASTA EL ÁPEX- DESPUÉS DE LA FIJACIÓN EN FORMOL AL 10%. NÓTESE EL INTENSO COLOR VERDE DEL INFILTRADO MIOCÁRDICO AMARILLO, VIRADO AL VERDE POR LA ACCIÓN DEL FORMOL.
 |
| BLOG 139. FOTO 8 .- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
 |
| BLOG 139. FOTO 9 .- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
 |
| BLOG 139. FOTO 10 .- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
 |
| BLOG 139 Foto 11.-. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FOTO 7.-
IMMERSIÓN EN SOLUCIÓN DE DTT (DL-DITHIOTHREITOL).
REACTIVO PARA OXIDACIÓN Y REDUCCIÓN: REDUCCIÓN DE PROTEÍNAS.
DTT= 1,4 DITHIOTREITOL (C4H10O2S2). DIMERCAPTO-2,3 BUTANEDIOL; DTT;
1,4-DITHIO-DL-THREITOL; CLELAND'S REAGENT; DL-THREO-1,4-DIMERCAPTO-2,3-BUTANEDIOL.
AN EXCELLENT REAGENT FOR MANTAINING SH GROUPS IN REDUCED STATE;
QUANTITATIVELY REDUCES DISULFIDES.
MERCK D5545.
LA INMERSIÓN DE LAS REBANADAS CARDIACAS EN UNA SOLUCIÓN DE DTT PROVOCÓ EL VIRADO DEL COLOR VERDE POST-FORMÓLICO HACIA EL AMARILLO, TAL COMO SE HABÍA VISUALIZADO DURANTE LA AUTOPSIA.
EL EFECTO PROVOCADO POR EL POTENTE AGENTE DTT CONFIRMABA LA SOSPECHA DE QUE EL INFILTRADO CARDIACO AMARILLENTO, DETECTADO DURANTE LA AUTOPSIA, PODÍA CORRESPONDER A BILIRRUBINA. EL VIRADO AL VERDE, POSTFORMÓLICO, DESPERTÓ LA SOSPECHA DE QUE SE TRATABA DE UN EFECTO OXIDANTE DEL FORMOL (FORMALDEHIDO) SOBRE LA BILIRRUBINA HACIA BILIVERDINA.
 |
| BLOG 139. Foto 12.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
DL-DITHIOTHREITOL. DTT.
DTT= 1,4 DITHIOTREITOL (C4H10O2S2). DIMERCAPTO-2,3 BUTANEDIOL; DTT;
1,4-DITHIO-DL-THREITOL; CLELAND'S REAGENT; DL-THREO-1,4-DIMERCAPTO-2,3-BUTANEDIOL.
AN EXCELLENT REAGENT FOR MANTAINING SH GROUPS IN REDUCED STATE;
QUANTITATIVELY REDUCES DISULFIDES.
MERCK D5545.
A= AUTOPSIA.
1.-ASPECTO DEL DEPÓSITO DE BILIRRUBINA OBSERVADO DURANTE LA NECROPSIA.
F= FIJACIÓN EN FORMOL AL 10%.
2.-OXIDACIÓN DE LA BILIRRUBINA A BILIVERDINA POR EL FORMALDEHIDO AL 10%.
3.-ASPECTO DE LA PIGMENTACIÓN DESPUÉS DE LA REDUCCIÓN EN DTT DURANTE 12 HORAS. NÓTESE EL VIRADO DEL COLOR VERDE AL AMARILLENTO POR LA REDUCCIÓN DE LA BILIVERDINA A BILIRRUBINA.
4.- DESPUÉS DE 24 HORAS EN DTT, EL COLOR AMARILLENTO SE HACE MÁS EVIDENTE.
LA INVESTIGACIÓN MICROSCÓPICA
 |
| BLOG 139. FOTO 13.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A FOTO 9.-
ASPECTO A PEQUEÑO AUMENTO DEL CAMPO MICROSCÓPICO CORRESPONDIENTE AL DEPÓSITO PIGMENTARIO, EL CUAL APARECE INTENSAMENTE COLOREADO DE AZUL CON LA COLORACIÓN TRICRÓMICA DE MASSON.
NÓTESE LA DISTRIBUCIÓN GEOGRÁFICA -MESOCÁRDICA Y CIRCUNFERENCIAL- DE LA INFILTRACIÓN MACROSCÓPICA CORRESPONDIENTE AL DEPÓSITO PIGMENTARIO, ASI COMO EL INTENSO COLOR AZUL DE LA ZONA.
|
 |
| BLOG 139. FTO 14.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FOTO 10.- A MEDIANO AUMENTO SE PUEDE COMPROBAR QUE EL ÁREA PIGMENTADA SE MUESTRA CONSTITUIDA POR UN TEJIDO QUE POSEE UNA DISPOSICIÓN "ZONAL" EN FORMA DE NÓDULOS ESFEROIDALES QUE HA SUSTITUIDO AL TEJIDO MIOCÁRDICO NORMAL.
 |
| BLOG 139. FOTO 15.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FOTO Nº 11.- MORFOLOGÍA DEL PATRÓN MICROSCÓPICO DE LA NECROSIS MIOCÁRDICA. A LA IZQUIERDA LA GRASA EPICÁRDICA.
LA ZONA NECRÓTICA APARECE TEÑIDA DE AZUL INTENSO.
NÓTESE QUE LA NECROSIS POSEE UN PATRÓN DE DISTRIBUCIÓN MESOCÁRDICO.
 |
| BLOG 139. FOTO 16.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
A LA IZQUIERDA DEL CAMPO, EL EPICARDIO. HACIA LA DERECHA, EL ENDOCARDIO.
PROF. GARFIA.A
 |
| BLOG 139. FOTO 17.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
LA SORPRESA
FOTO 18.-
SE PUEDE DISTINGUIR AHORA -NO SIN CIERTA SORPRESA- QUE LAS ÁREAS NODULARES CONFLUENTES SE ENCUENTRAN CONSTITUIDAS POR FOCOS DE NECROSIS MIOCÁRDICA -CUYOS MIOCARDIOCITOS NECRÓTICOS PRESENTAN UNA INTENSA COLORACIÓN AZUL (BASÓFILA) CON EL TRICRÓMICO DE MASSON.
 |
| BLOG 139 Foto 19.-. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
LA MIOCARDITIS AGUDA
FOTO 14.-
JUNTO A LA FRONTERA DEL ÁREA NECRÓTICA -EN EL INTERSTICIO MIOCÁRDICO- SE PUEDE VER LA APROXIMACIÓN LEUCOCITARIA, EN FORMA DE COLUMNA QUE CAMINA POR EL TEJIDO CONECTIVO INTERSTICIAL, HACIA LAS 12 DE LA ESFERA HORARIA.
 |
| BLOG 139. Foto 20.-HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FOTO 13.-
LA COLUMNA LEUCOCITARIA INFILTRANDO EL TEJIDO CONECTIVO PERINECRÓTICO.
 |
| BLOG 139. Foto 21.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A FOTO 14 |
EN AZUL, LAS BANDAS O LÍNEAS DE UNIÓN DESMOSÓMICAS (LÍNEAS Z).
 |
| BLOG 139. Foto 22.- HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
EN LA FRONTERA DE LA NECROSIS
FOTO 23.-
MIOCARDIOCITOS EN PROCESO DE DESINTEGRACIÓN NECRÓTICA -EN LA PARTE SUPERIOR- LOCALIZADOS EN LA PERIFERIA DEL ÁREA DE NECROSIS ESTABLECIDA, SITUADA EN LA PARTE INFERIOR DE LA FOTOGRAFÍA.
 |
| BLOG 139 Foto 24.-HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
EN EL FOCO DE NECROSIS.
M
FOTO 25 .-
SE VEN ALGUNAS BANDAS DE CONTRACCIÓN Y RESTOS DE LA ESTRIACIÓN EN ALGUNOS MIOCARDIOCITOS. PREDOMINA LA INTENSA BASOFILIA EN LA MAYORÍA DE LOS MIOCARDIOCITOS NECRÓTICOS.
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
EN EL CENTRO DEL ÁREA NECRÓTICA SE CONSERVA UN MIOCARDIOCITO QUE PRESENTA BANDAS DE HIPERCONTRACCIÓN EOSINÓFILAS EN EL CITOPLASMA.
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A |
FOTO 28.-
EXISTE UNA GRAN DIFICULTAD PARA PONER DE MANIFIESTO, MICROSCÓPICAMENTE, LOS DEPÓSITOS PIGMENTARIOS DE BILIRRUBINA.
EN LA FOTOGRAFÍA SE DISTINGUEN -DE MANERA EVIDENTE- UN GRUPO DE PIGMENTOS, DE COLOR PARDO AMARILLENTO, LOCALIZADOS A LAS 12 DE LA ESFERA DEL RELOJ.
EXISTE UNA SEVERA DEFORMACIÓN Y HEMÓLISIS ERITROCITARIA.
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A. FOTO 20 |
DEPÓSITOS DE BILIRRUBINA SEÑALADOS POR LAS FLECHAS.
M=MIOCARDIOCITOS NECRÓTICOS.
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A. FOTO 21 |
LAS TINCIONES CON HEMATOXILINA-EOSINA-FLOXINA DEMUESTRAN LA NECROSIS DE COAGULACIÓN DE LOS MIOCARDIOCITOS, LA MIOCITOLISIS Y LA PRESENCIA DE INCLUSIONES CITOPLASMÁTICAS BASÓFILAS -ALGUNAS DE LAS CUALES SUGIEREN UNA ETIOLOGÍA BACTERIANA.
 |
| BLOG 139. HERZIKTERUS. HISTOPATOLOGIA FORENSE PRACTICA. PROF. GARFIA.A.
FOTO 31.- Inclusiones citoplásmicas basófilas en numerosos miocardiocitos
que podrían corresponder a bacterias.
|
BIBLIOGRAFÍA CONSULTADA
Schmorl, G.-
Zur kenntniss der Ikterus Neonatorum, insbesondere der dabei umftretenden Gehirnveranderungen. Verhandlung Deutsche Patologische Gesellschaft. 6: 109. 1903
Fang, J., Akaike, T and Maeda.H
Antiapoptotic role of heme oxygenase (HO) and the potential of HO as a target in anticancer treatment. Apoptosis 2004; 9:27-35.
Turkel SB.-
Autopsy findings associated with neonatal hyperbilirubinemia.
Clin Perinatol. 1990 Ju; 17 (2): 381-396.
Masini, E et al.-
Hme Oxygenase-1 and the Ischemia-Reperfusion Injury in the Rat Heart.
Exp Biol Med 228:546-549, 2003.
Wu TW et al.-
Albumin-bound bilirubins protect human ventricular myocites against oxyradical damage.
Biochem Cell Biol 69: 683-688. 1991.
Raju VS et al.-
Cardioselective overexpression of HO-1 prevents I/R-induced cardiac dysfunction and apoptosis.
Am J Physiol Heart Circ Physiol 283: H688-H694. 2002.
Agradecimientos
A la Dra. María José Haro, por la ayuda prestada en la traducción al inglés.
Suscribirse a:
Entradas (Atom)











{kind=link}